

Mild "Perolight" in the treatment of acne disease
T. Bendelian
Medical Corporation "Evex", Tbilisi, Georgia
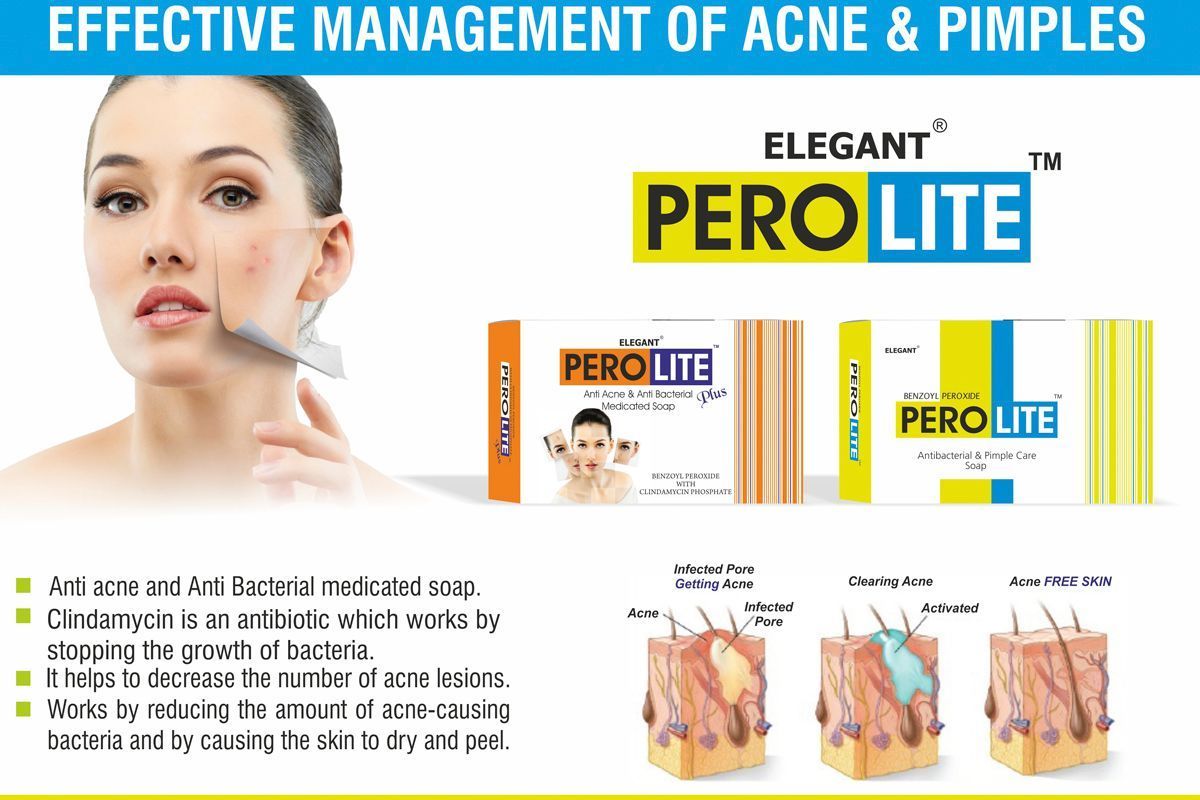
This article presents data from a clinical study on the efficacy of soap branded as "Perolight", which contains benzoyl peroxide, and "Perolight Plus", which contains benzoyl peroxide and clindamycin, for the local treatment of acne.
The studies, conducted in clinics in Georgia from May 2017 to April 2018, involved 120 patients with mild to moderate acne (according to the dermatological acne index). The soap "Perolight" and "Perolight Plus" were used twice a day (morning and evening) as monotherapy for patients with mild acne and in combination with a gel containing benzoyl peroxide for severe cases.
After just 1 month of using the soap, most patients (83%) with mild acne showed a decrease in the dermatological acne index, while patients with moderate acne saw a reduction of more than 60%.
Improvement was particularly rapid with the use of "Perolight Plus" in patients with pronounced pustular elements. Based on the results of the study, it can be concluded that the soap "Perolight" has sufficient therapeutic activity and is well tolerated by patients during both monotherapy and combination therapy for acne.
Furthermore, it can be successfully used during the summer period. All of this provides grounds to recommend the soap "Perolight" for widespread use in clinical practice.
Keywords: Acne, soap "Perolight", benzoyl peroxide.
Acne is a polymorphic multifactorial disease characterized by genetic predisposition. According to statistical data, among dermatoses, it is the most common skin pathology—up to 85% of people aged 12 to 25 suffer from acne [2]. This phenomenon is particularly widespread among residents of megacities, who are more susceptible to the negative effects of environmental factors.
Acne affects approximately 85% of adolescents (of which 25% have severe forms of the disease). Active forms of acne are diagnosed in 20% of adults, and about 50% of women regularly report outbreaks of lesions. Acne belongs to the group of diseases known as psychosomatic dermatoses, which are associated with the issue of "defect of appearance," lowering a person's self-esteem and causing depression and anxiety. Despite the availability of modern treatment methods, acne remains one of the most common dermatoses—the incidence is not only not decreasing but is noticeably increasing.
The pathogenetic factors contributing to the development of acne include:
- hypersecretion of sebaceous glands,
- changes in the qualitative parameters of sebum and epidermal lipids;
- pathological keratinization of the follicular canal in the infundibular part (between the sebaceous gland and the surface of the epidermis);
- intense colonization of Propionibacterium acnes in sebaceous glands;
- development of an inflammatory reaction in the perifollicular zones [1].
In some cases, topical agents are the first line of treatment for acne, especially at the onset of the disease and in mild forms of adolescent acne. In 2002, recommendations were developed and an algorithm for pathogenetic treatment of patients with various forms of acne was created (XX World Congress of Dermatology, Paris, 2002), where the first-choice medications are topical retinoids, benzoyl peroxide, antibiotics, and azelaic acid, which affect the processes of keratinization (keratinization and desquamation), reduce sebum production, enhance the proliferation of skin epithelial cells, and provide certain anti-inflammatory effects [4].
Today, one of the effective methods for treating acne is benzoyl peroxide, which contains a residue of benzoic acid. When applied to the skin, this lipophilic compound undergoes a chemical reaction with oxygen and breaks down into two substances—peroxide and benzoic acid. The latter substance is inactive and is not absorbed into the skin. The active peroxide destroys bacteria by affecting their walls and also reduces the level of fatty acids secreted by the skin, thereby preventing inflammation. In addition, the agent has a therapeutic effect—damaging keratinized cells and preventing skin peeling.
Benzoyl peroxide exhibits nonspecific antimicrobial activity against P. acnes, Staphylococcus epidermidis, and some other microorganisms and has been used in dermatology since the 20th century [3]. Being a powerful oxidizer, it penetrates follicles better than other topical agents, contacts the membrane of P. acnes, and has a bactericidal effect. When benzoyl peroxide breaks down, benzoic acid is formed, which acts bacteriostatically, does not accumulate in tissues, has no systemic effects, and is excreted from the body unchanged. The anti-inflammatory action of benzoyl peroxide is achieved by inactivating free radical forms of oxygen in the area of inflammation, destroying free fatty acids, and reducing their concentration. The comedolytic action of benzoyl peroxide is explained by the fact that, due to its chemical structure, it is a strong oxidizer that suppresses the inflammatory process and the formation of comedones [4].
The advantage of preparations containing this substance is that they do not cause the emergence of resistant strains of bacteria.
For one year, 120 patients with acne were monitored, with the severity determined based on the number of comedones, pustules, papules, and nodules. In the presence of single elements, the dermatological acne index was less than 5 points (mild severity), with a moderate number—6-15 points (moderate severity), and with a large number—more than 15 points. In 78 (65%) patients, mild acne was diagnosed, and in 42 (35%)—moderate severity. For mild acne, the soap "Perolight" was prescribed twice a day (morning and evening) as monotherapy and in combination with a gel containing benzoyl peroxide. In this case, patients used the soap in the evening and the gel in the morning. Regardless of the severity of the process, but in the presence of multiple pustular elements, the soap "Perolight Plus," which contains clindamycin, was prescribed.
The average treatment course in most cases lasted 5-7 weeks. Only in three patients with moderate acne was the course extended to 8-9 weeks. The effectiveness of therapy was assessed by changes in the dermatological acne index one month after the start and 6-8 weeks after the end of treatment.
The safety of the soap "Perolight," objective and subjective data regarding its effectiveness, as well as an assessment of the dynamics of the clinical course of acne during treatment, were analyzed.
After just 1 month of using the soap, most patients with mild acne showed a decrease in the dermatological acne index (83%), while in moderate cases, the index decreased by more than 60%. Improvement was particularly rapid with the use of "Perolight Plus" in patients with pronounced pustular elements. All patients tolerated the soap well: 80% rated the tolerance as very good, and 20% as good. An important point was the absence of side effects related to sun exposure during the summer period. All patients with mild acne rated the effectiveness of the soap as very good and were completely satisfied with the results of the treatment. Most patients with moderate acne were satisfied with the treatment results, with only 3 cases not achieving complete clinical effect within 2 months. It is also important that the quality of life of patients with acne is one of the factors of effectiveness, as the disappearance of clinical manifestations positively affects their overall and mental state.
Based on the results of the study, it can be concluded that the soap "Perolight" has sufficient therapeutic activity and is well tolerated by patients during both monotherapy and combination therapy for acne. Furthermore, it can be successfully used during the summer period. All of this provides grounds to recommend the soap "Perolight" for widespread use in clinical practice.
References
1. Kiselova N.V. The Role of Histocompatibility Antigens in the Development of Various Forms of Acne and Correction Methods: Author's Abstract of the Dissertation ... Candidate of Medical Sciences; 14.00.11.- Moscow, 2001.- 22 p.
2. Cunliffe W.J. New Approaches To Acne Treatment.- London: Martin Dunitz, 2004.- 56 p.
3. Perry A., Lambert P. Propionibacterium acnes: Infection beyond the skin // Expert Review of Anti-infective Therapy.- 2011.- Vol. 9, N 12.- P. 1149-1156. doi: 10.1586 / eri.11.137.
4. Savage L.J., Layton A.M. Treating acne vulgaris: systemic, local and combination therapy // Expert Rev. Clin. Pharmacol.-2010.- Vol. 13.- P. 563-580. doi: 10.1586 / ecp.10.27.
5. Zaenglein A.L., Pathy A.L., Schlosser B.J. et al. Guidelines of care for the management of acne vulgaris // J. Am. Acad. Dermatol.- 2016.- Vol. 74, N 5.- P. 945-973. doi: 10.1016 / j. jaad.2015.12.037.
News
All news
With the first warm days, you want to spend more time in the sun. The spring sun rays seem soft and safe, but during this period, the skin is particularly vulnerable after winter. A weakened protective barrier and dryness make it more sensitive to ultraviolet light. Therefore, sun protection in spring is just as important as in summer.

Skincare is more than just aesthetics. It's a daily ritual that reminds us of self-love, of taking time for ourselves, of comfort. That's why quality skincare is a universal gift, suitable for any occasion: a birthday, a professional holiday, an anniversary, or simply as a gesture of attention without a reason.
We have gathered beauty ideas that not only bring pleasant emotions but also deliver real results.
Pigment spots are an unpleasant dermatological problem influenced by various factors, such as the sun, hormonal and age-related changes affecting the production of melanin, leading to hyperpigmentation. How does this acid work in skincare dermocosmetics? Read on in the material.

PSORIASIS IS AN IMMUNOLOGICALLY MEDIATED DISEASE THAT MANIFESTS WITH SYMPTOMS ON THE SKIN AND SOMETIMES IN THE JOINTS.
Psoriasis affects 2% to 3% of the population of Ukraine.
Treatment of psoriasis at the modern stage includes a complex of systemic and topical agents, as well as physiotherapy methods, including the use of water procedures (hydrotherapy), which are prescribed to patients individually depending on the stage of the dermatosis, accompanying somatic diseases, etc.

In the field of manicure and pedicure, the hands of the master are their main tool. They constantly come into contact with aggressive chemicals, nail dust, dyes, and other irritants.
If you have previously used retinoids and AHA acids, you probably know that retinoids work deep within the layers of the skin. In contrast, AHA acids only work on the upper layers of the dermis.

Scalp problems, such as discomfort, itching, and flaking skin, significantly affect a person's emotional state.

pigmentation is a fairly common problem that can appear at any stage of life. It occurs due to uneven distribution of melanin — the pigment responsible for the color of our skin, hair, and eyes.

Historically, it has been the case that a person always strives to maintain youthfulness for longer and to have firm and toned skin, but unfortunately, the loss of skin elasticity is a natural part of the aging process. It affects the condition of the skin, its firmness, and elastin.

Azelaic acid is a natural component that has anti-inflammatory, antibacterial, and comedolytic properties.





